EXHIBIT 99.1
Published on June 28, 2024
Exhibit 99.1
Topline Results: RZ402 - 201 Phase 2 Study in Patients with Diabetic Macular Edema (DME) May 21, 2024
This presentation, like many written and oral communications presented by Rezolute and our authorized officers, may contain certain forward - looking statements regarding our prospective performance and strategies within the meaning of Section 27A of the Securities Act and Section 21E of the Securities Exchange Act of 1934, as amended. We intend such forward - looking statements to be covered by the safe harbor provisions for forward - looking statements contained in the Private Securities Litigation Reform Act of 1995 and are including this statement for purposes of said safe harbor provisions. Forward - looking statements, which are based on certain assumptions and describe future plans, strategies, and expectations of Rezolute , are generally identified by use of words such as "anticipate," "believe," "estimate," "expect," "intend," "plan," "project," "prove," "potential," "seek," "strive," "try," or future or conditional verbs such as "predict," "could," "may," "likely," "should," "will," "would," or similar expressions. These forward - looking statements include but are not limited to statements regarding the RZ402 study, the ability of RZ402 to become an effective treatment for diabetic macular edema, the effectiveness or future effectiveness of RZ402 to become an effective treatment for diabetic macular edema, and statements regarding clinical trial timelines for RZ402. Our ability to predict results or the actual effects of our plans or strategies is inherently uncertain. Accordingly, actual results may differ materially from anticipated results. Readers are cautioned not to place undue reliance on these forward - looking statements, which speak only as of the date of this release. Except as required by applicable law or regulation, Rezolute undertakes no obligation to update these forward - looking statements to reflect events or circumstances that occur after the date on which such statements were made. Important factors that may cause such a difference include any other factors discussed in our filings with the SEC, including the Risk Factors contained in the Rezolute’s Annual Report on Form 10 - K and Quarterly Reports on Form 10 - Q, which are available at the SEC’s website at www.sec.gov. You are urged to consider these factors carefully in evaluating the forward - looking statements in this release and are cautioned not to place undue reliance on such forward - looking statements, which are qualified in their entirety by this cautionary statement. Forward - Looking Statements | 2

Introduction
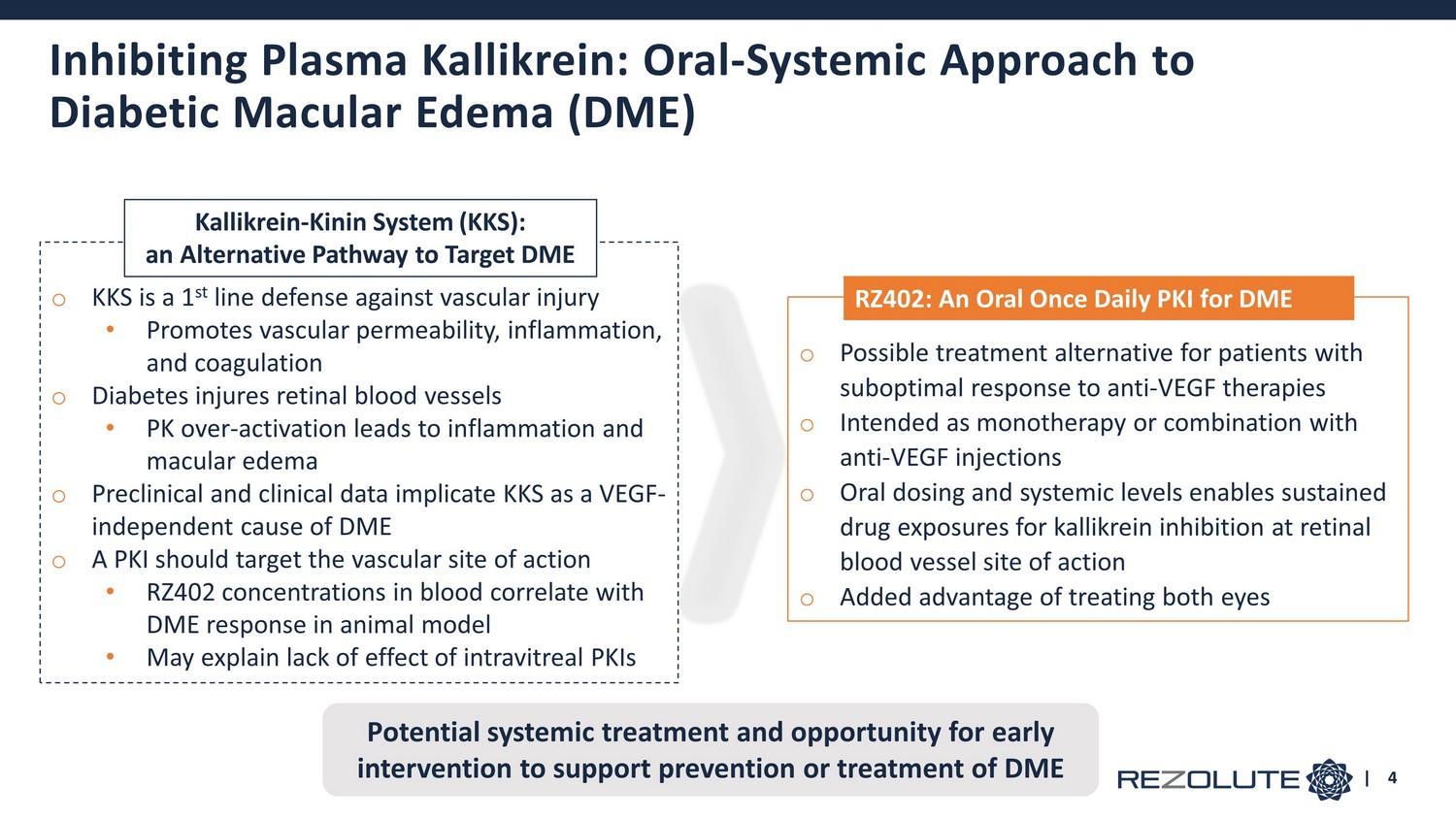
o KKS is a 1 st line defense against vascular injury • Promotes vascular permeability, inflammation, and coagulation o Diabetes injures retinal blood vessels • PK over - activation leads to inflammation and macular edema o Preclinical and clinical data implicate KKS as a VEGF - independent cause of DME o A PKI should target the vascular site of action • RZ402 concentrations in blood correlate with DME response in animal model • May explain lack of effect of intravitreal PKIs o Possible treatment alternative for patients with suboptimal response to anti - VEGF therapies o Intended as monotherapy or combination with anti - VEGF injections o Oral dosing and systemic levels enables sustained drug exposures for kallikrein inhibition at retinal blood vessel site of action o Added advantage of treating both eyes | 4 Kallikrein - Kinin System (KKS): an Alternative Pathway to Target DME RZ402: An Oral Once Daily PKI for DME Potential systemic treatment and opportunity for early intervention to support prevention or treatment of DME Inhibiting Plasma Kallikrein: Oral - Systemic Approach to Diabetic Macular Edema (DME)
RZ402 Phase 2 Study Topline Results
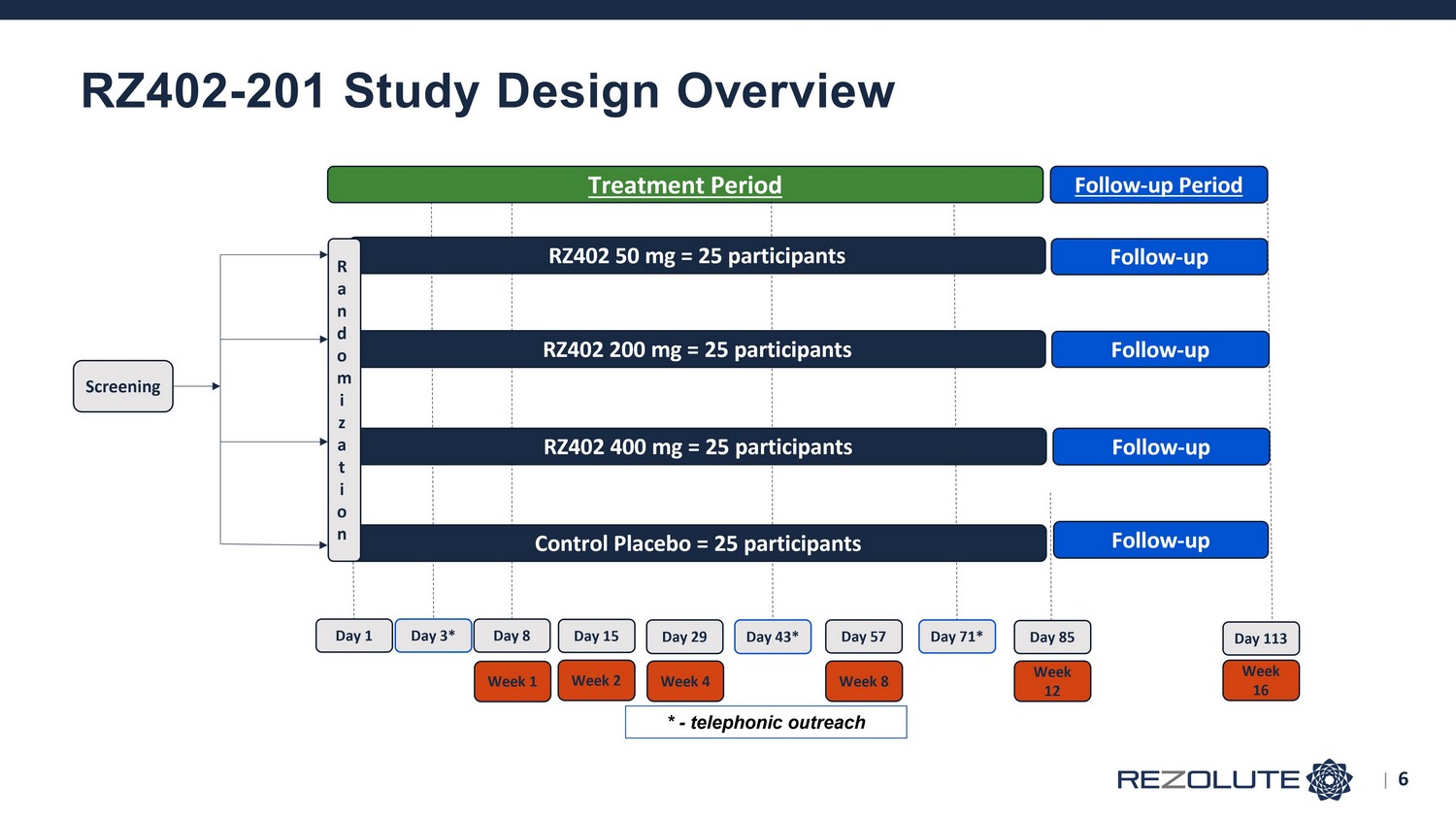
RZ402 - 201 Study Design Overview | 6
o Primary • Safety, including AEs and SAEs, ocular exams, and systemic evaluations (e.g. vitals, ECG, labs) • Efficacy – Change in Central Subthreshold Thickness ( CST) from baseline compared to placebo • A recognized and objective Phase 2 anatomic marker of macular edema o Secondary • Change in best corrected visual acuity (BCVA) from baseline compared to placebo • Change in Diabetic Retinopathy Severity Score (DRSS) score compared to placebo • Exploratory and not expected to change in a 3 - month study • Repeat - dose PK profile of RZ402 • Fellow eye evaluation (in evaluable eyes not treated with anti - VEGF) Endpoints | 7
o Mild to moderate non - proliferative diabetic retinopathy with center - involved DME o No more than 3 anti - VEGF injections previously • None within 8 weeks of randomization o CST of ≥320 microns in males and ≥305 microns in females o BCVA ≤78 letters on Early Treatment Diabetic Retinopathy Study (ETDRS) o Stable glycemic control Key Eligibility Criteria | 8
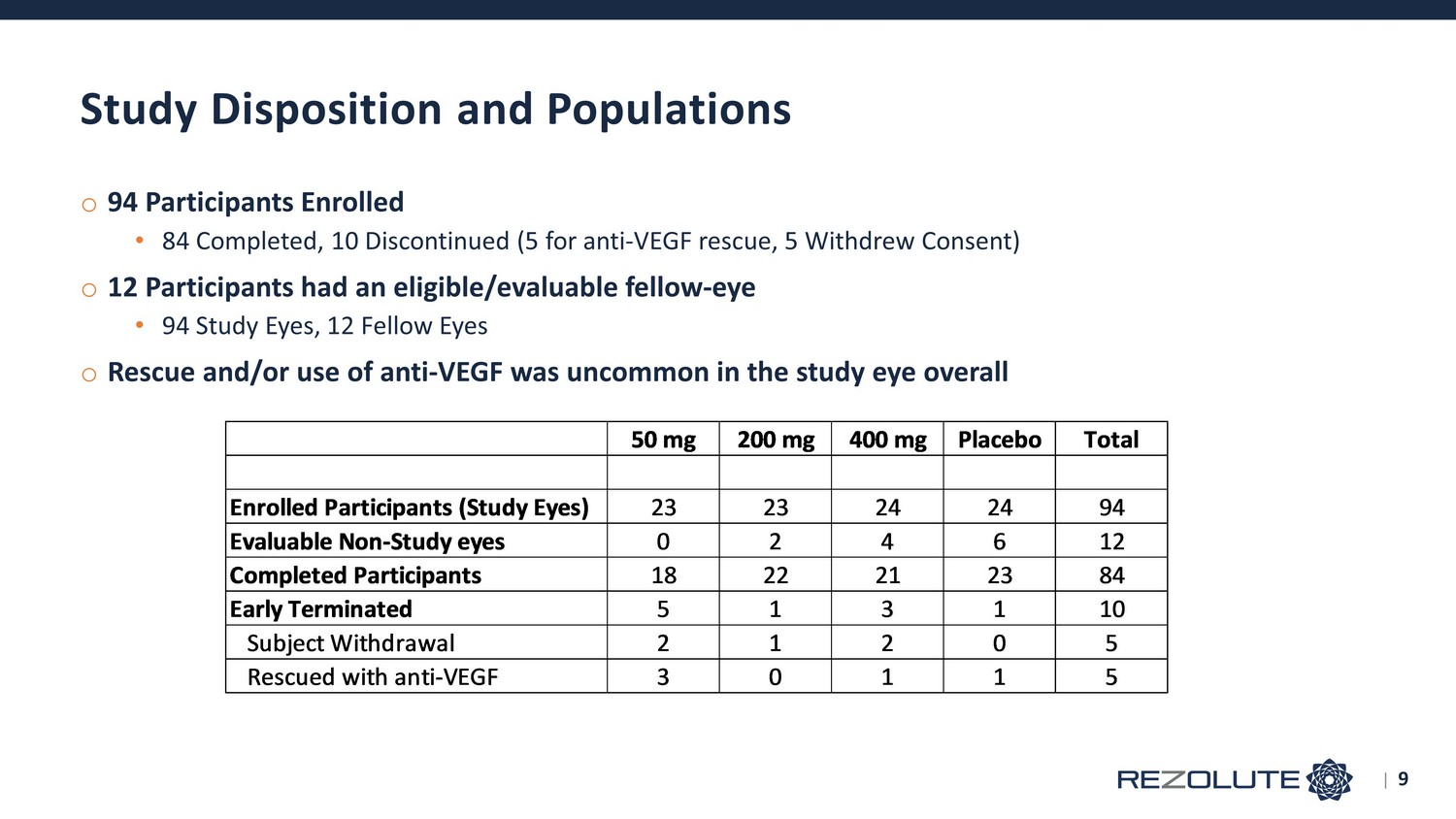
o 94 Participants Enrolled • 84 Completed, 10 Discontinued (5 for anti - VEGF rescue, 5 Withdrew Consent) o 12 Participants had an eligible/evaluable fellow - eye • 94 Study Eyes, 12 Fellow Eyes o Rescue and/or use of anti - VEGF was uncommon in the study eye overall Study Disposition and Populations 50 mg 200 mg 400 mg Placebo Total Enrolled Participants (Study Eyes) 23 23 24 24 94 Evaluable Non-Study eyes 0 2 4 6 12 Completed Participants 18 22 21 23 84 Early Terminated 5 1 3 1 10 Subject Withdrawal 2 1 2 0 5 Rescued with anti-VEGF 3 0 1 1 5 | 9
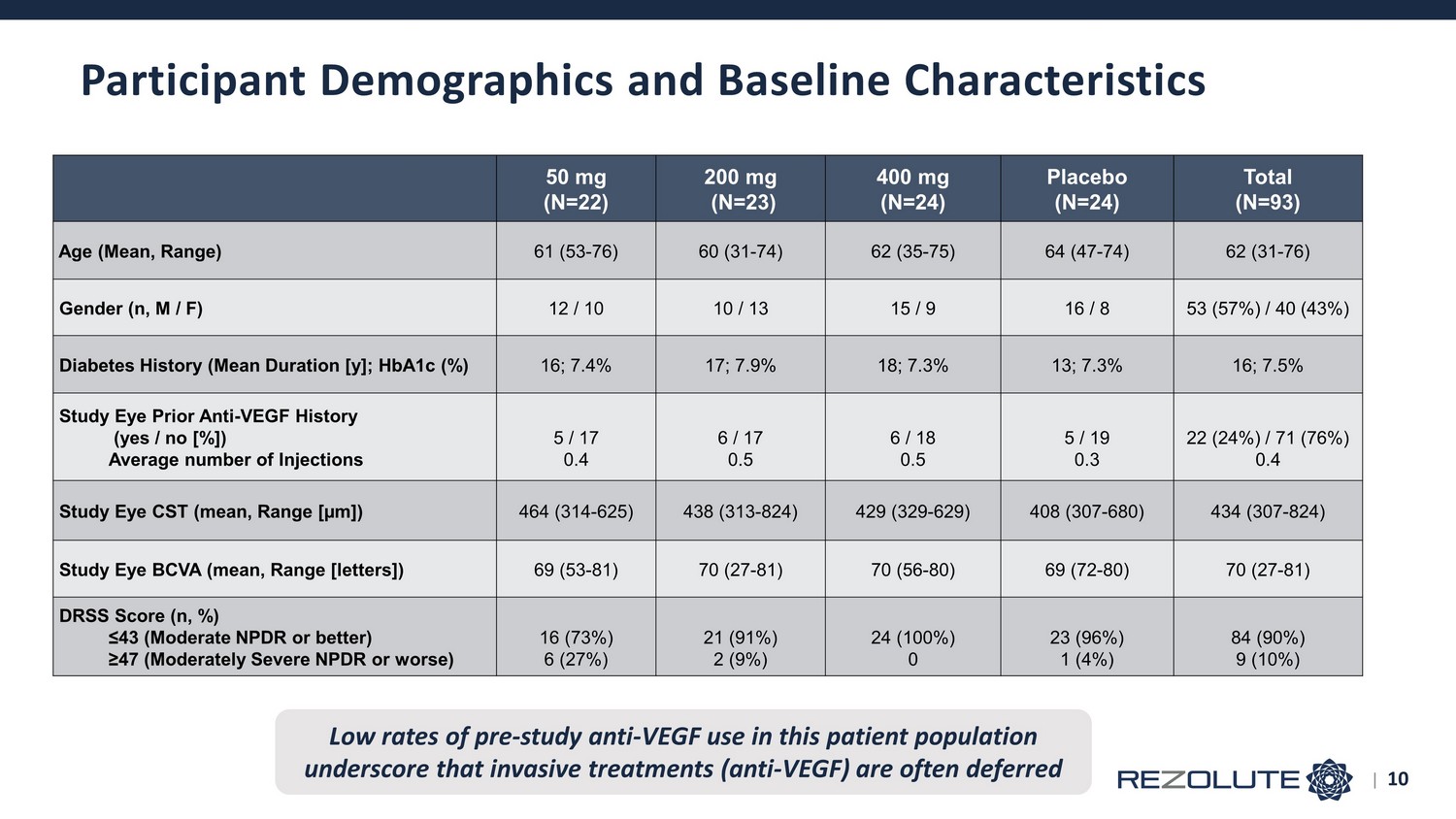
Participant Demographics and Baseline Characteristics 50 mg (N=22) 200 mg (N=23) 400 mg (N=24) Placebo (N=24) Total (N=93) Age (Mean, Range) 61 (53 - 76) 60 (31 - 74) 62 (35 - 75) 64 (47 - 74) 62 (31 - 76) Gender (n, M / F) 12 / 10 10 / 13 15 / 9 16 / 8 53 (57%) / 40 (43%) Diabetes History (Mean Duration [y]; HbA1c (%) 16; 7.4% 17; 7.9% 18; 7.3% 13; 7.3% 16; 7.5% Study Eye Prior Anti - VEGF History (yes / no [%]) Average number of Injections 5 / 17 0.4 6 / 17 0.5 6 / 18 0.5 5 / 19 0.3 22 (24%) / 71 (76%) 0.4 Study Eye CST (mean, Range [µm]) 464 (314 - 625) 438 (313 - 824) 429 (329 - 629) 408 (307 - 680) 434 (307 - 824) Study Eye BCVA (mean, Range [letters]) 69 (53 - 81) 70 (27 - 81) 70 (56 - 80) 69 (72 - 80) 70 (27 - 81) DRSS Score (n, %) ≤43 (Moderate NPDR or better) ≥47 (Moderately Severe NPDR or worse) 16 (73%) 6 (27%) 21 (91%) 2 (9%) 24 (100%) 0 23 (96%) 1 (4%) 84 (90%) 9 (10%) Low rates of pre - study anti - VEGF use in this patient population underscore that invasive treatments (anti - VEGF) are often deferred | 10
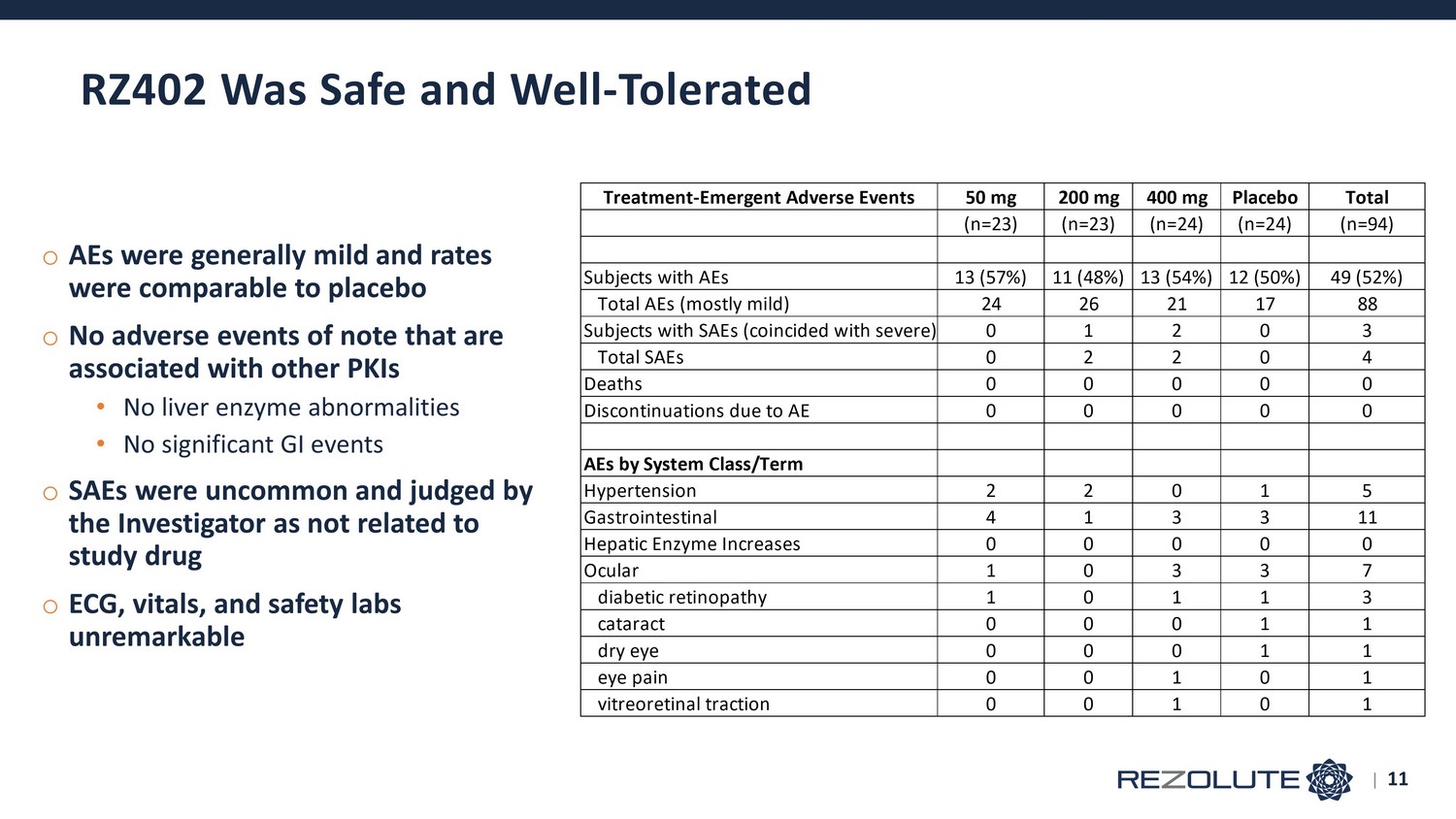
o AEs were generally mild and rates were comparable to placebo o No adverse events of note that are associated with other PKIs • No liver enzyme abnormalities • No significant GI events o SAEs were uncommon and judged by the Investigator as not related to study drug o ECG, vitals, and safety labs unremarkable RZ402 Was Safe and Well - Tolerated Treatment-Emergent Adverse Events 50 mg 200 mg 400 mg Placebo Total (n=23) (n=23) (n=24) (n=24) (n=94) Subjects with AEs 13 (57%) 11 (48%) 13 (54%) 12 (50%) 49 (52%) Total AEs (mostly mild) 24 26 21 17 88 Subjects with SAEs (coincided with severe) 0 1 2 0 3 Total SAEs 0 2 2 0 4 Deaths 0 0 0 0 0 Discontinuations due to AE 0 0 0 0 0 AEs by System Class/Term Hypertension 2 2 0 1 5 Gastrointestinal 4 1 3 3 11 Hepatic Enzyme Increases 0 0 0 0 0 Ocular 1 0 3 3 7 diabetic retinopathy 1 0 1 1 3 cataract 0 0 0 1 1 dry eye 0 0 0 1 1 eye pain 0 0 1 0 1 vitreoretinal traction 0 0 1 0 1 | 11
o Dose - dependent but not dose - proportional increases in concentrations o Expected concentrations were achieved and profile supports once daily oral dosing o Concentration which resulted in a 90% reduction in macular edema in rodent models of DME (EC90) was exceeded at all dose levels in the present study • Assuming equivalent potency translation to humans, near maximal kallikrein inhibition was likely achieved across all doses Preliminary Pharmacokinetics | 12
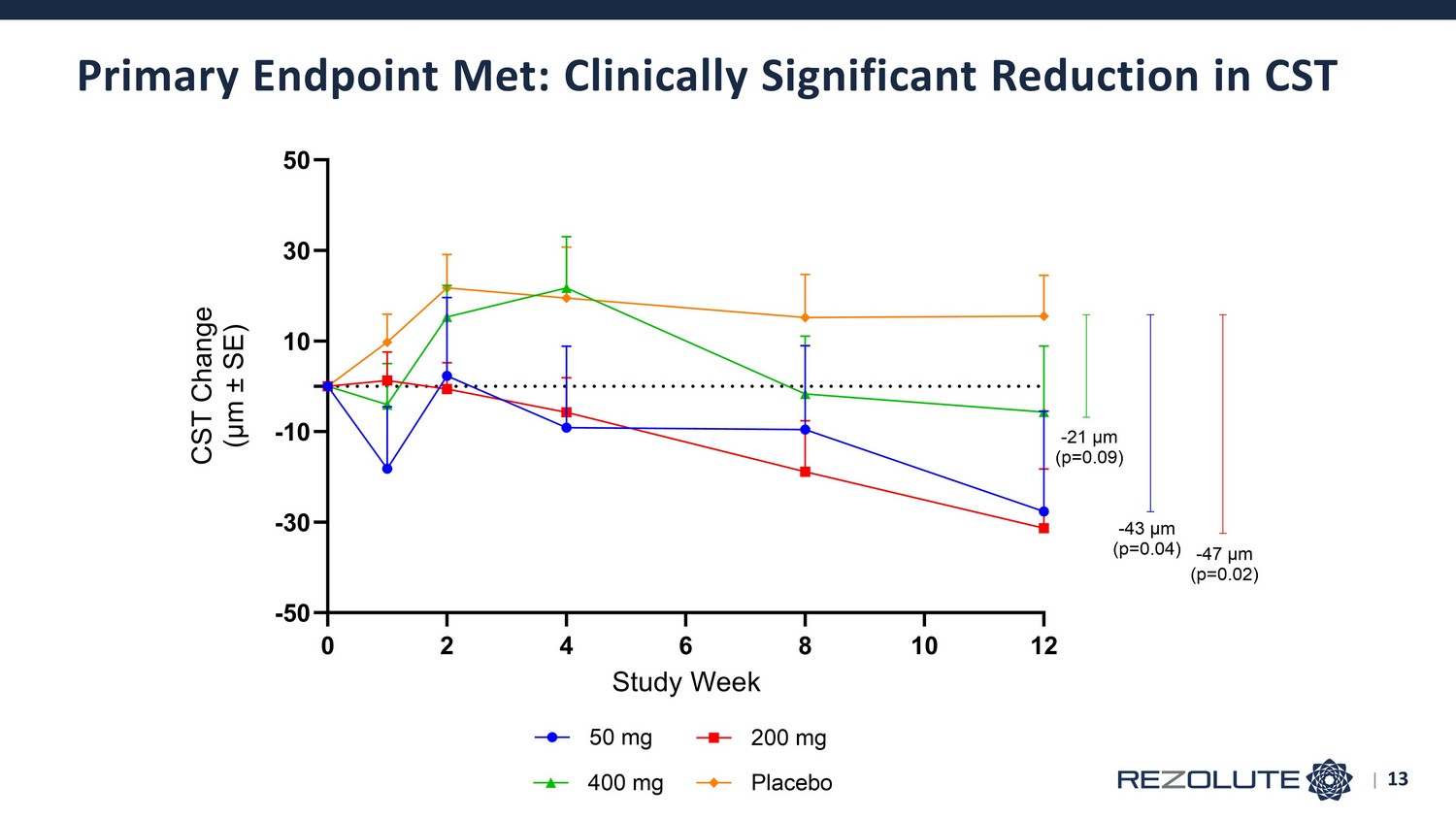
Primary Endpoint Met: Clinically Significant Reduction in CST 0 2 4 6 8 10 12 -50 -30 -10 10 30 50 Study Week C S T C h a n g e ( μ m ± S E ) 50 mg 200 mg 400 mg Placebo -47 μm (p=0.02) -21 μm (p=0.09) -43 μm (p=0.04) | 13
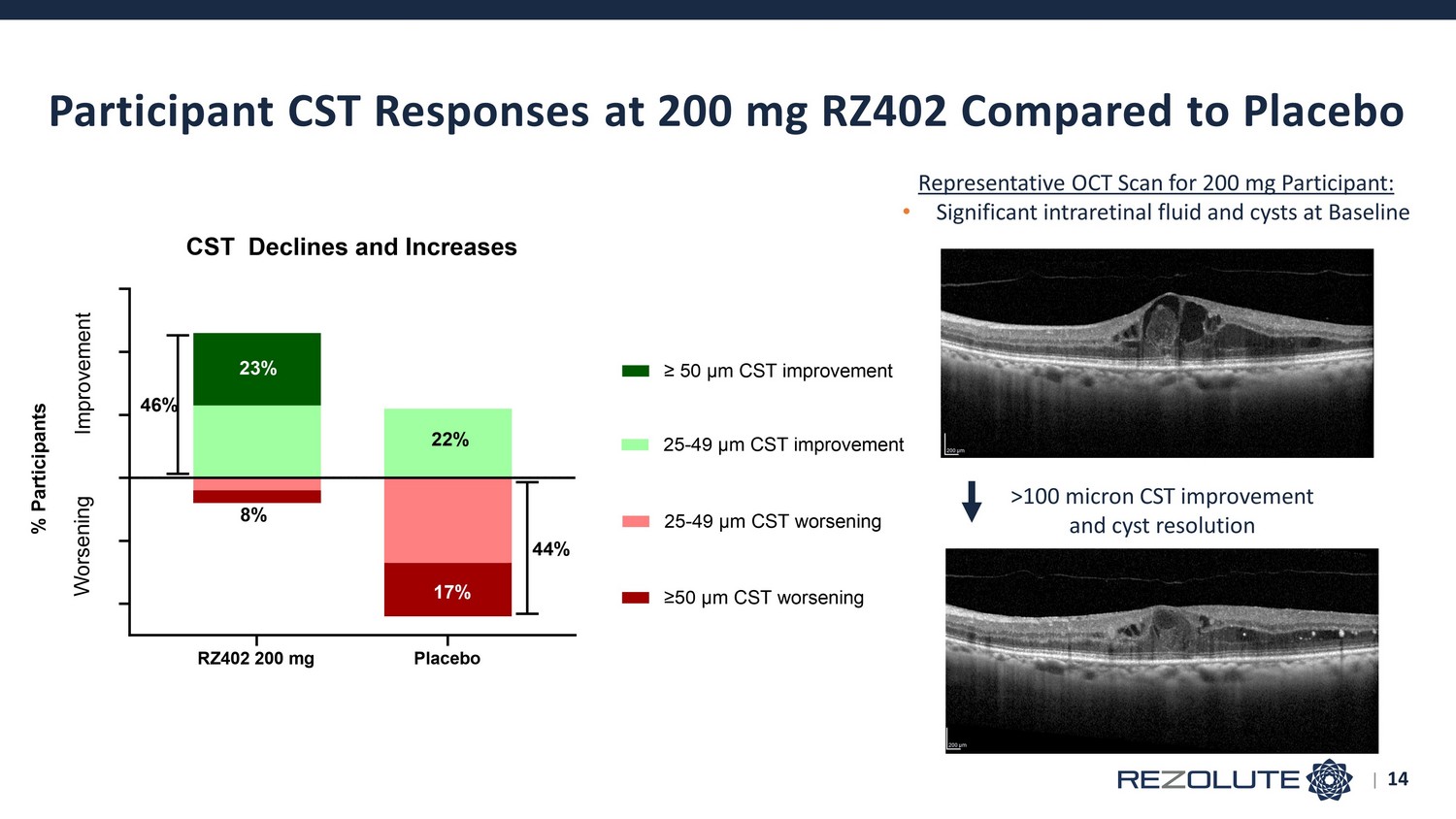
Participant CST Responses at 200 mg RZ402 Compared to Placebo | 14 RZ402 200 mg Placebo CST Declines and Increases W o r s e n i n g % P a r t i c i p a n t s I m p r o v e m e n t 25-49 μm CST worsening ≥50 μm CST worsening 25-49 μm CST improvement ≥ 50 μm CST improvement 23% 46% 8% 22% 44% 17% Representative OCT Scan for 200 mg Participant: • Significant intraretinal fluid and cysts at Baseline >100 micron CST improvement and cyst resolution
o Achieved good systemic exposure and safe and well - tolerated o First PKI and oral therapy of any class to demonstrate a CST improvement in patients with DME • CST improved significantly in Study Eye at all doses compared to placebo (up to ~50 microns) • A pre - specified sub - analysis by CST severity indicates that CST improvements were even larger (~75 microns) in subset of patients with more baseline edema (CST values ≥ 400 microns) • CST declined in most patients who received 200 mg RZ402, including clinically significant improvements from baseline in more than 20% of participants, compared to none in placebo, with high rates of worsening o Maximal response at 200 mg likely explained by drug saturation of plasma kallikrein activity o Vision is not expected to improve or correlate with CST changes over a 3 - month study • Observed improvements in CST predictive of visual improvements in a longer duration study o Five RZ402 treated participants at 200 mg (20%) experienced a 1 - step improvement in DRSS compared to 1 participant in placebo o Minority of non - study eyes retrospectively met eligibility criteria, and anti - VEGF use was not restricted in the non - study eye • It is likely that both eyes would benefit simultaneously, in a study designed to assess this o Results support advancement into late - stage development (longer duration Phase 2b/3 studies) Additional Endpoints and Summary of Results | 15
Thank You

Appendix June 28, 2024
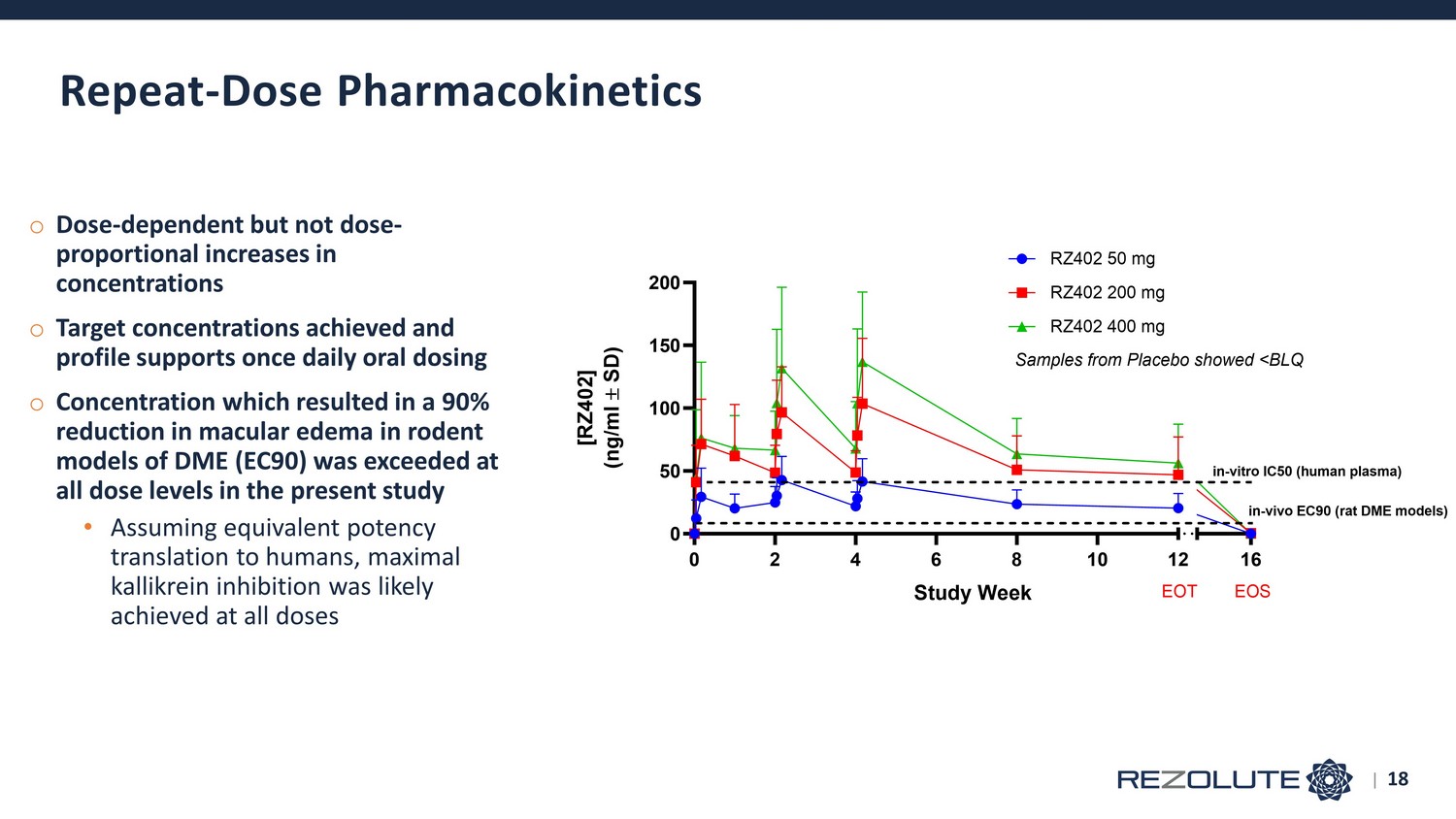
o Dose - dependent but not dose - proportional increases in concentrations o Target concentrations achieved and profile supports once daily oral dosing o Concentration which resulted in a 90% reduction in macular edema in rodent models of DME (EC90) was exceeded at all dose levels in the present study • Assuming equivalent potency translation to humans, maximal kallikrein inhibition was likely achieved at all doses Repeat - Dose Pharmacokinetics | 18 0 2 4 6 8 10 12 0 50 100 150 200 16 Study Week [ R Z 4 0 2 ] ( n g / m l S D ) RZ402 50 mg RZ402 200 mg RZ402 400 mg EOT EOS Samples from Placebo showed <BLQ in-vitro IC50 (human plasma) in-vivo EC90 (rat DME models)
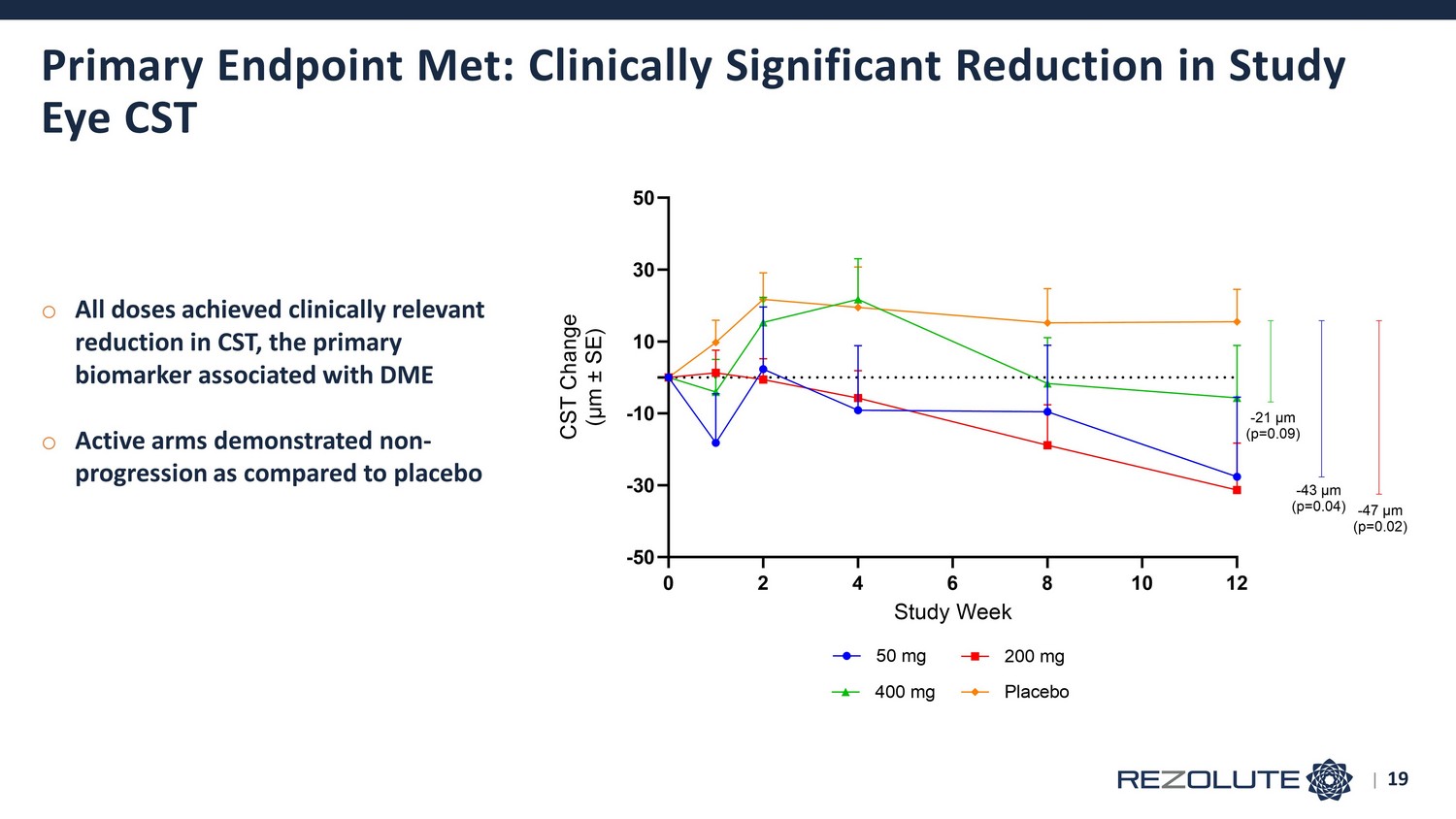
Primary Endpoint Met: Clinically Significant Reduction in Study Eye CST 0 2 4 6 8 10 12 -50 -30 -10 10 30 50 Study Week C S T C h a n g e ( μ m ± S E ) 50 mg 200 mg 400 mg Placebo -47 μm (p=0.02) -21 μm (p=0.09) -43 μm (p=0.04) | 19 o All doses achieved clinically relevant reduction in CST, the primary biomarker associated with DME o Active arms demonstrated non - progression as compared to placebo
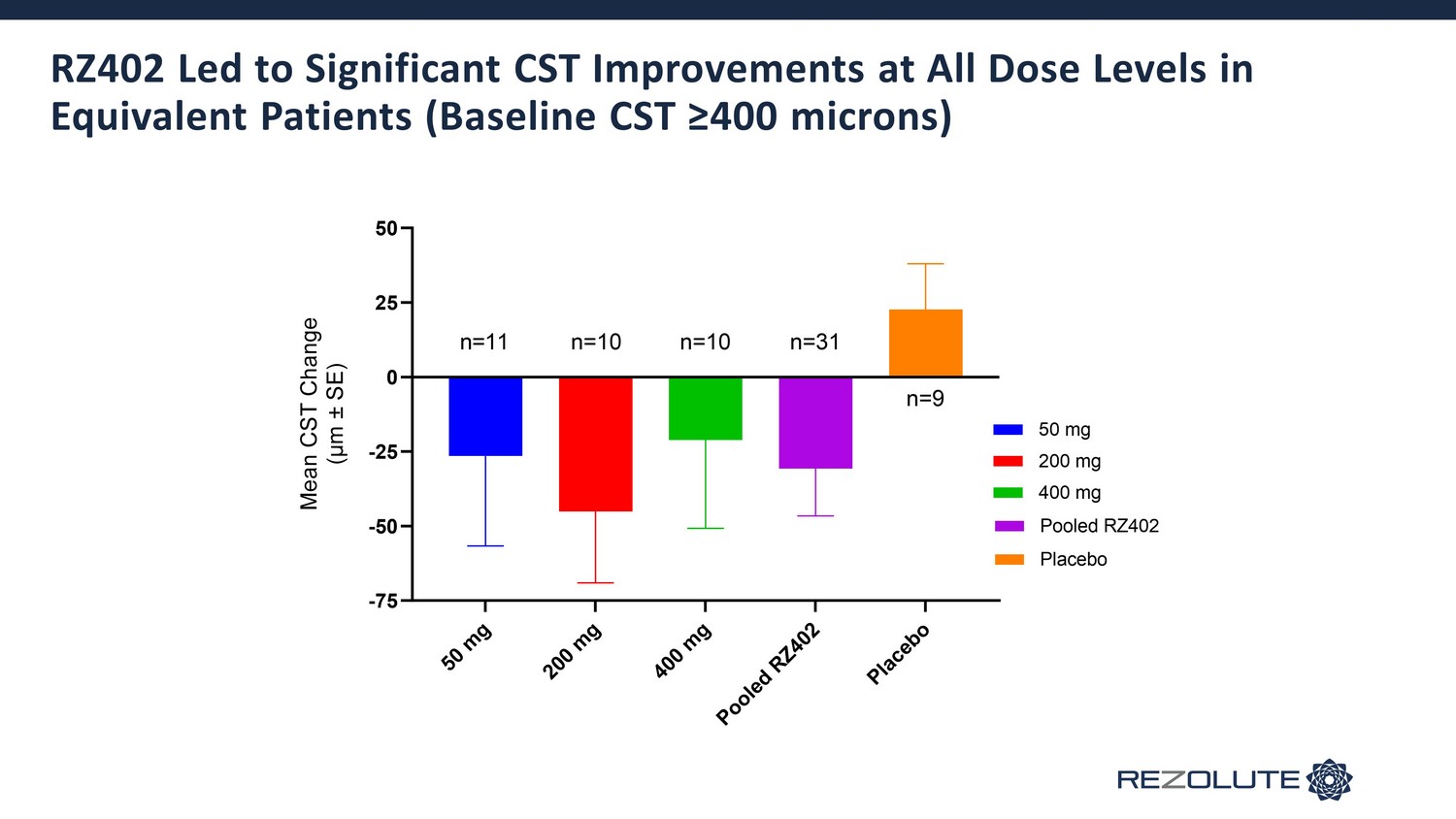
RZ402 Led to Significant CST Improvements at All Dose Levels in Equivalent Patients (Baseline CST ≥400 microns) 5 0 m g 2 0 0 m g 4 0 0 m g P o o l e d R Z 4 0 2 P l a c e b o -75 -50 -25 0 25 50 M e a n C S T C h a n g e ( μ m ± S E ) 50 mg Pooled RZ402 200 mg 400 mg Placebo n=11 n=10 n=10 n=31 n=9
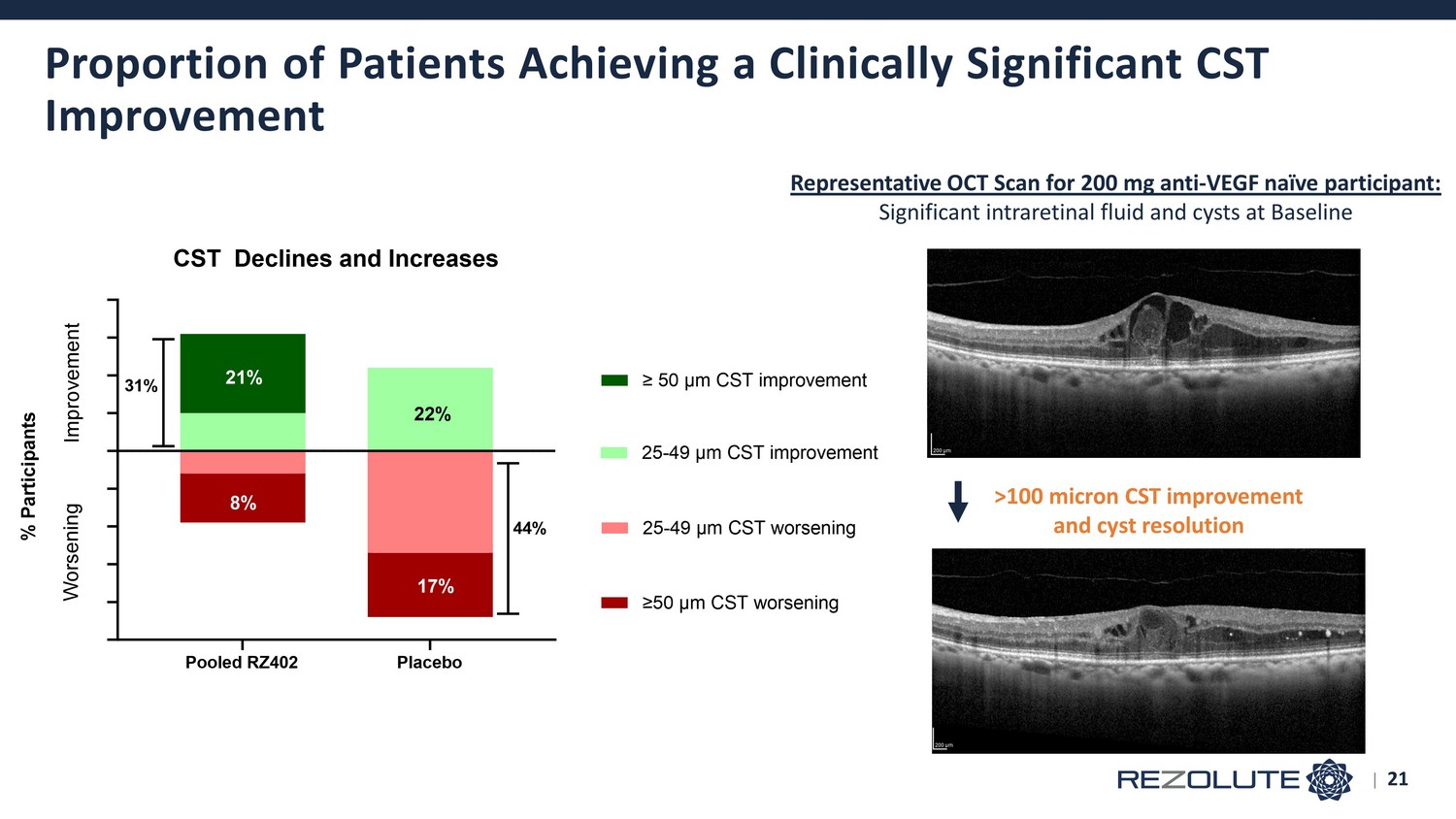
Proportion of Patients Achieving a Clinically Significant CST Improvement | 21 Pooled RZ402 Placebo CST Declines and Increases W o r s e n i n g % P a r t i c i p a n t s I m p r o v e m e n t 25-49 μm CST worsening ≥50 μm CST worsening 25-49 μm CST improvement ≥ 50 μm CST improvement 21% 31% 8% 22% 44% 17% Representative OCT Scan for 200 mg anti - VEGF naïve participant: Significant intraretinal fluid and cysts at Baseline >100 micron CST improvement and cyst resolution
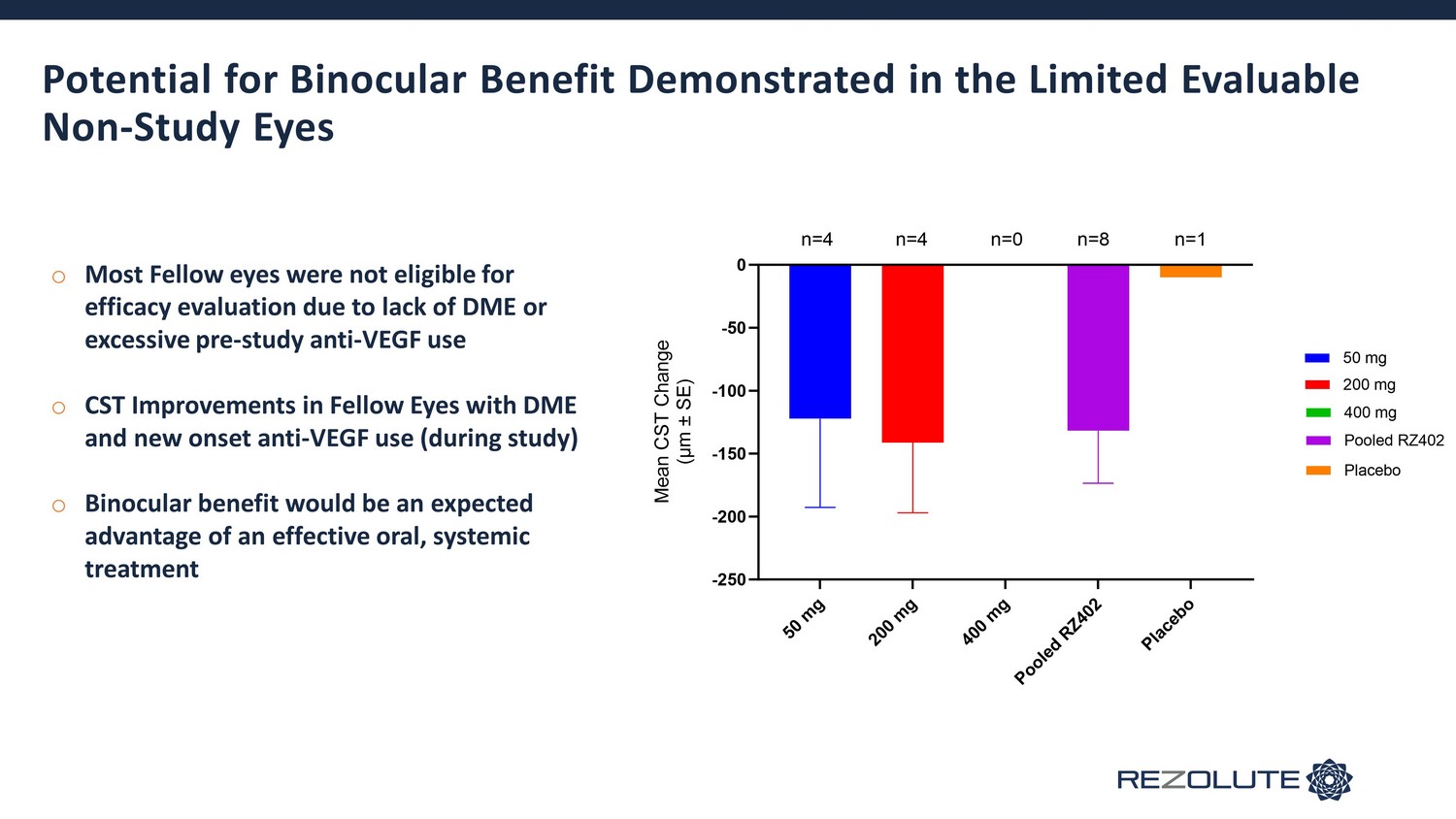
Potential for Binocular Benefit Demonstrated in the Limited Evaluable Non - Study Eyes 5 0 m g 2 0 0 m g 4 0 0 m g P o o l e d R Z 4 0 2 P l a c e b o -250 -200 -150 -100 -50 0 M e a n C S T C h a n g e ( μ m ± S E ) 200 mg 400 mg Placebo 50 mg Pooled RZ402 n=4 n=4 n=8 n=1n=0 o Most Fellow eyes were not eligible for efficacy evaluation due to lack of DME or excessive pre - study anti - VEGF use o CST Improvements in Fellow Eyes with DME and new onset anti - VEGF use (during study) o Binocular benefit would be an expected advantage of an effective oral, systemic treatment
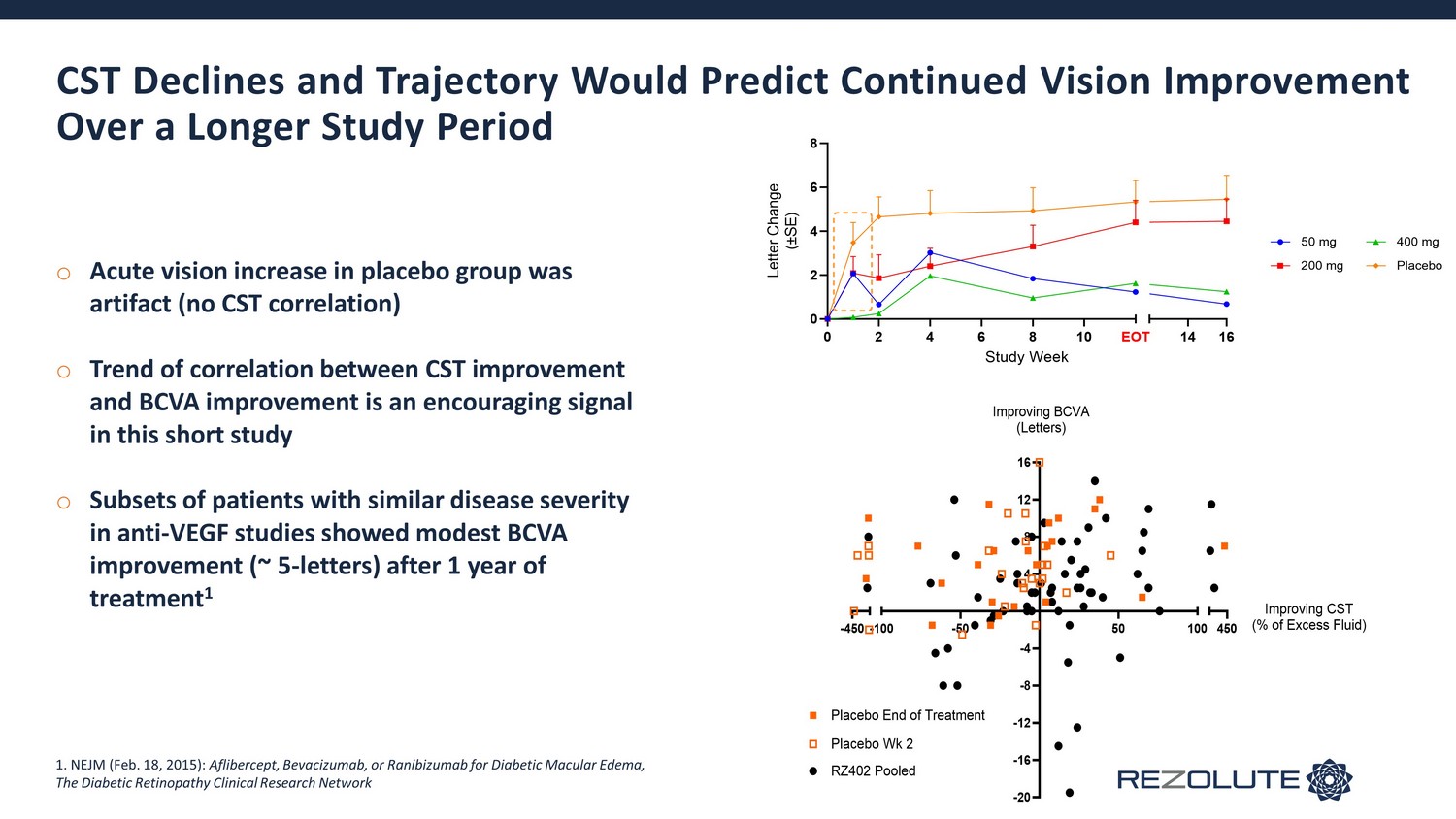
CST Declines and Trajectory Would Predict Continued Vision Improvement Over a Longer Study Period 0 2 4 6 8 10 0 2 4 6 8 14 16 Study Week L e t t e r C h a n g e ( ± S E ) 50 mg 200 mg 400 mg Placebo EOT -450 -20 -16 -12 -8 -4 4 8 12 16 -100 -50 50 100 450 Improving BCVA (Letters) Improving CST (% of Excess Fluid) Placebo End of Treatment Placebo Wk 2 RZ402 Pooled o Acute vision increase in placebo group was artifact (no CST correlation) o Trend of correlation between CST improvement and BCVA improvement is an encouraging signal in this short study o Subsets of patients with similar disease severity in anti - VEGF studies showed modest BCVA improvement (~ 5 - letters) after 1 year of treatment 1 1. NEJM (Feb. 18, 2015): Aflibercept, Bevacizumab, or Ranibizumab for Diabetic Macular Edema, The Diabetic Retinopathy Clinical Research Network